
Copper-Deficiency Anemia vs Iron-Deficiency Anemia
Author: VP Grewal, MD. 2021 March 21.
Copper is a trace mineral present in all organisms in nature, and is an essential trace mineral in humans. Copper is a component of a multitude of vital enzymes in the human body and helps with electron transport, energy production, and oxygen transportation.
Copper has been used in ancient medicine for thousands of years, and was the antiseptic of choice for the ancient Egyptian, Greeks, Aztecs, and Chinese. Ancient Hindu and Persian literature revealed many uses for copper to treat inflammation, arthritis, cancer, seizures, and even for healing broken bones. In 18th century France, copper tubs were used for 8 to 12 hour hot baths for the treatment of nervous diseases. In India, copper was referred to as “the destroyer of the whiteness of the skin”, most likely referring to treating anemia.
Iron deficiency results in diminished red blood cell production and is almost always caused by increased blood loss from the body, most commonly gastrointestinal or menstrual. Other causes include urinary blood loss, malabsorption, and poor oral intake. Symptoms of iron-deficiency anemia include chronic fatigue, poor exercise tolerance, shortness of breath, weakness, a fast resting heartbeat, heart palpitations, and pale skin.
The primary treatment for iron-deficiency anemia is oral therapy with ferrous sulfate tablets or intravenous iron in patients with malabsorption. Iron supplements have about a 50% success rate as a treatment for anemia thought to be caused by iron-deficiency. However, iron supplementation is not always necessary and may even lead to iron overload, especially in children who can overdose on iron supplements.
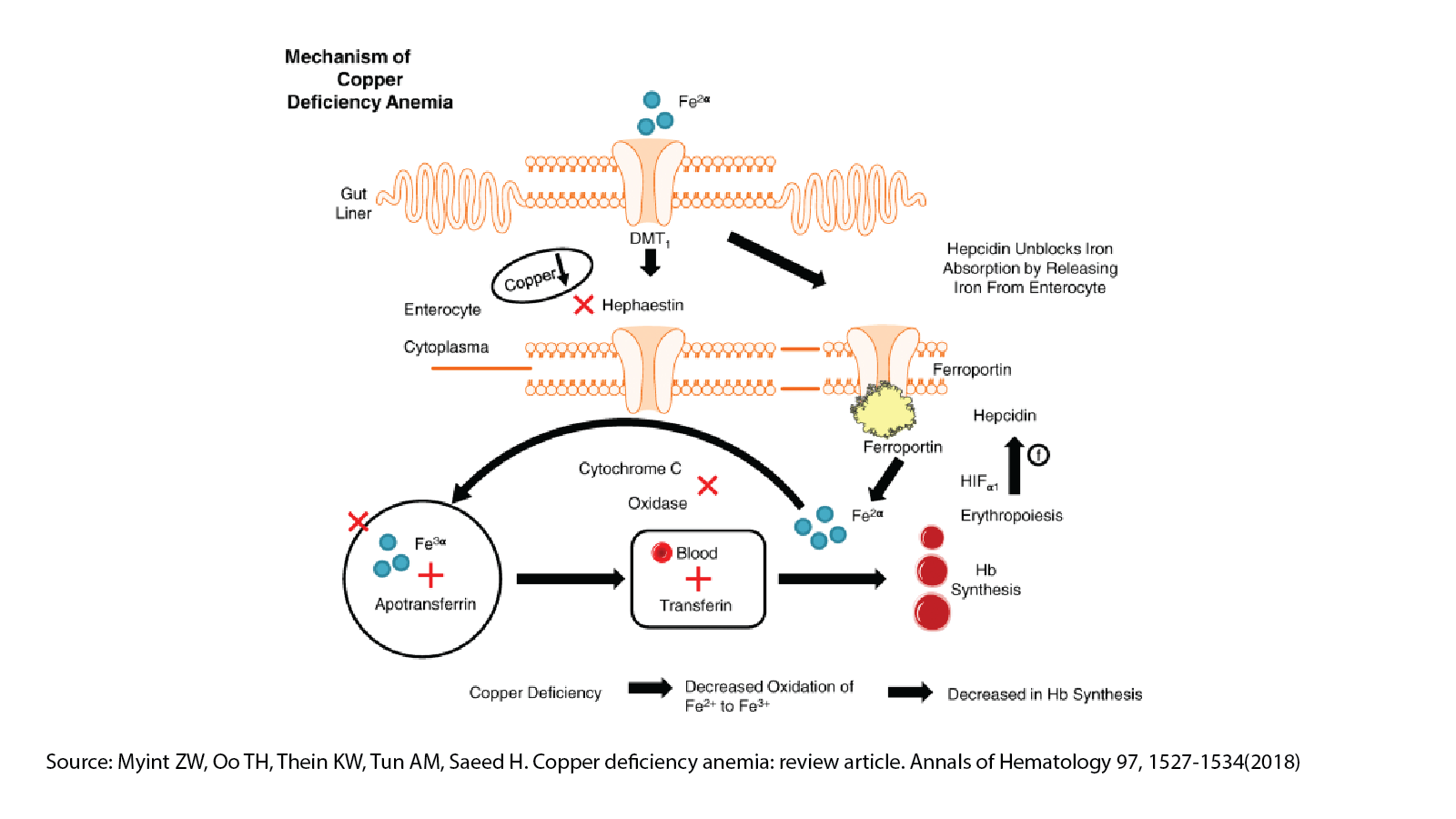
A neglected aspect in the treatment of suspected iron-deficiency anemia is the role of copper in hemoglobin synthesis. Although copper is not a major component of hemoglobin, it is a catalyst for the synthesis of hemoglobin. Copper is required for the intestinal absorption of iron, utilization of iron, and release of stored iron. Copper-deficiency is often the underlying cause for iron-deficiency anemia.
Copper-deficiency can also lead to iron overload, especially with the excessive intake of iron supplements. The accumulation of iron in the liver causes fatty liver disease, in the brain causes neurological disorders, in the pancreas causes diabetes, in the spleen causes anemia, and in the retina causes retinopathy.
Due to the interdependence of iron and copper in hemoglobin synthesis, it is common for physicians to misclassify copper-deficiency anemia as iron-deficiency anemia. Iron supplementation, in many cases, can block copper absorption further exacerbating copper deficiency.
The best food source of copper is beef liver. Vita Columbia’s Grass-Fed Beef Liver Chips contain 7.1 mg of copper per serving. Although the recommended daily intake (RDI) of copper is 0.9-1.3 mg, much higher amounts over 6 mg are needed for deprivation recovery. Organ meats such as liver also have a more optimal iron-zinc to copper ratio.
References:
Continue reading “Copper-Deficiency Anemia vs Iron-Deficiency Anemia”




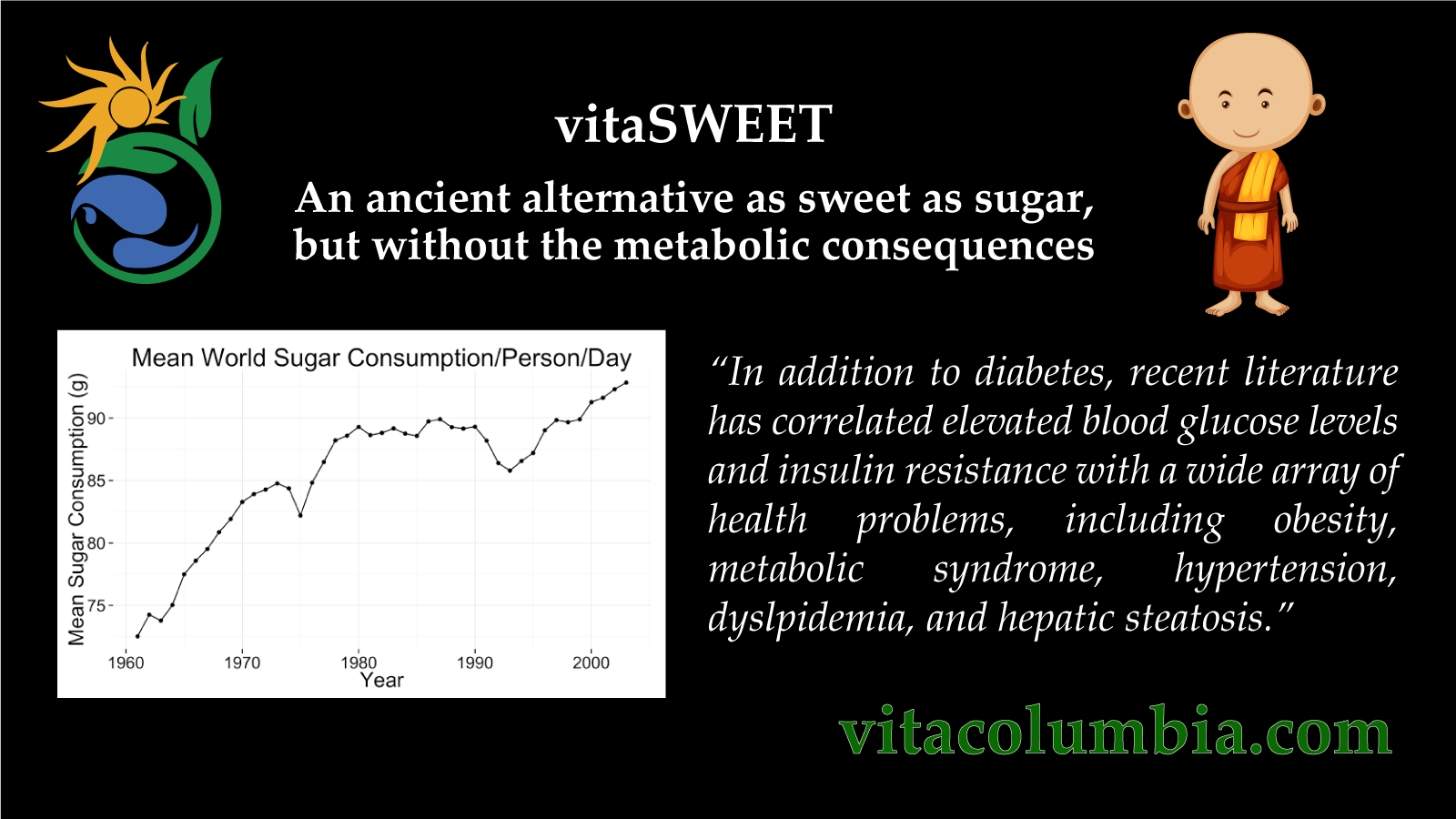
 World Sugar Consumption 1960 – 2006
World Sugar Consumption 1960 – 2006 Sales of sugary drinks by country
Sales of sugary drinks by country