
Dietary Sugar and the Childhood Obesity Epidemic
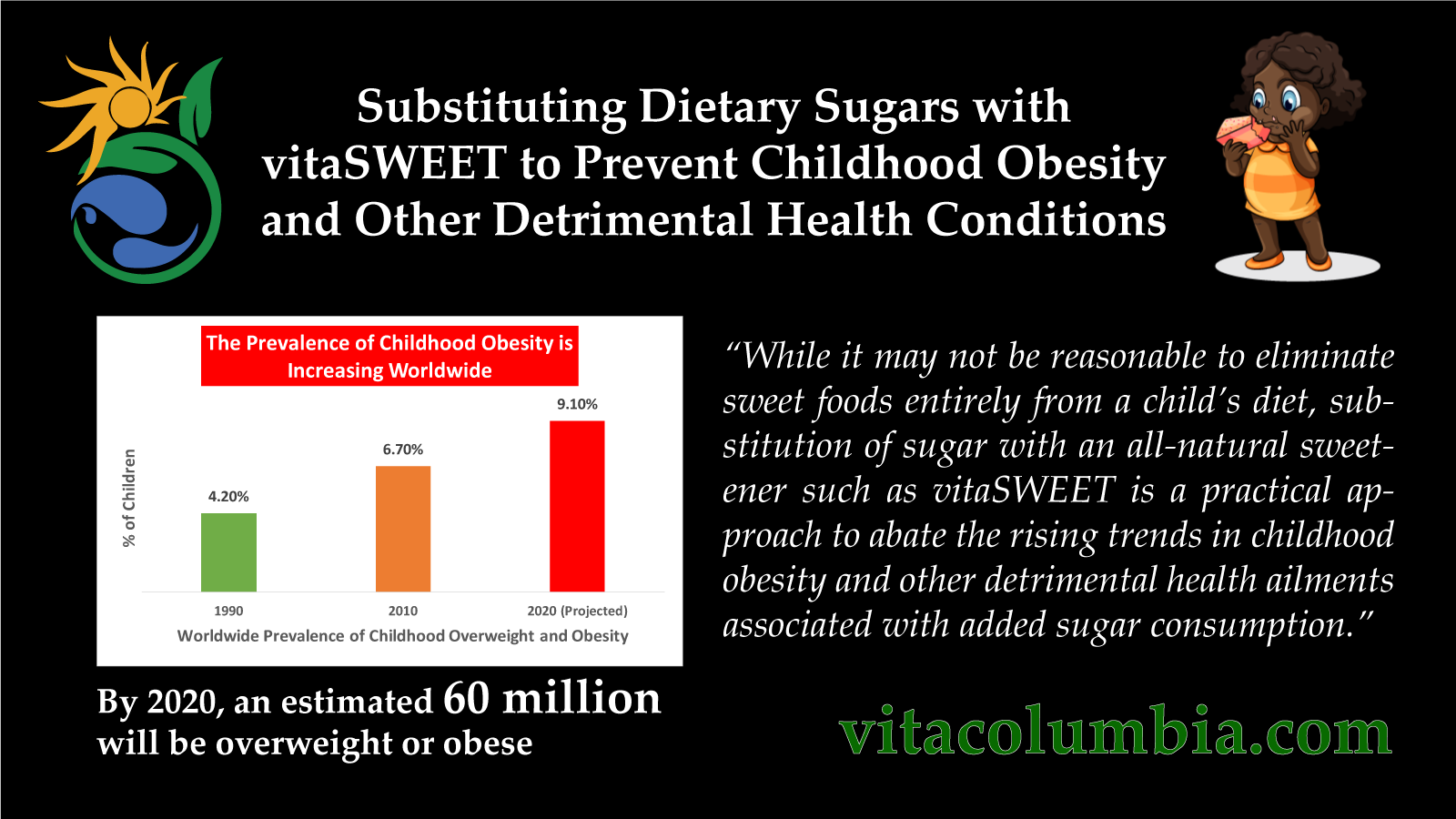
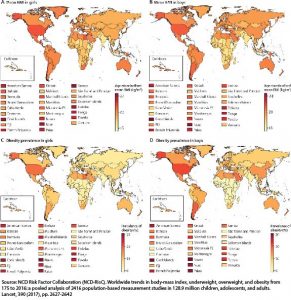
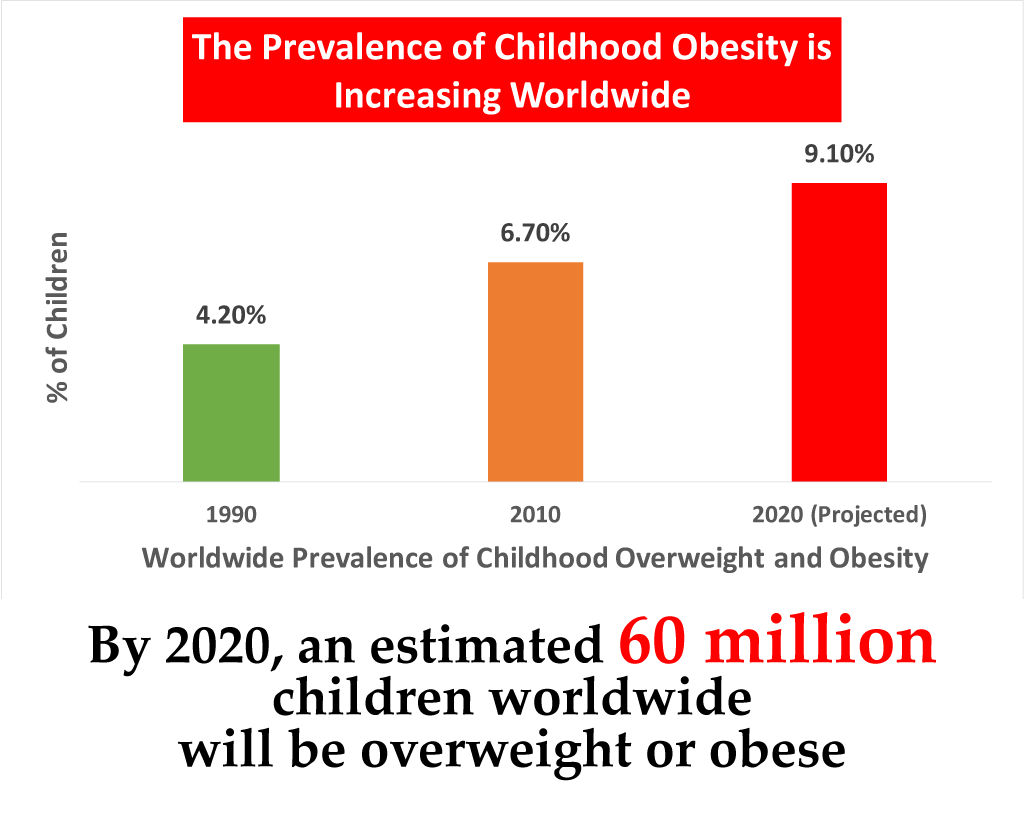
Preventing childhood obesity is vital due to its association with lifelong obesity, metabolic disorders such as type-2 diabetes mellitus and hypertriglyceridemia, obesity-related cancers, in addition to psychosocial repercussions and decreased educational attainment. From 1975 to 2016, mean BMI and obesity rates in children and adolescents aged 5-19 years have increased globally and in most regions.
Added sugar consumption is the primary factor associated with childhood obesity trends, in addition to being associated with other detrimental health conditions such as dental caries, asthma, altered lipid profiles, hypertension, and cancer. A 2019 analysis of data compiled from the Centers for Disease Control and Prevention (CDC) from 2011 to 2016 revealed 98% of American toddlers and 60% of infants consume added sugar in sweetened foods and beverages. Sweet bakery products were in the top 3 sources of added sugar for both toddlers and infants. Previous studies examining sugar intake in older children (aged 2-8 years) also reported sweet bakery products to be one of the top three sources for added sugar. Fruit drinks, yogurt, and sugar-sweetened beverages were other important sources of added sugar identified by researchers. In 2015, the World Health Organization (WHO) and the American Heart Association (AHA) recommended limiting added sugars consumption to <10% of total caloric intake for children aged 2 to 19 years. In 2017, the AHA released a statement advising children less than 2 years to old to avoid consuming added sugars entirely. The most recent analysis of CDC data revealed about 70% of American children older than 2 years exceed recommendations for added sugars intake.
Infants and children around the world exhibit a heightened preference for sweetness, most likely a biological underpinning to confer advantage in environments of scarcity. Moreover, emerging research has shown significant similarities in neurochemistry and behavior between consumption of added sugars and drug-like effects, including bingeing, craving, tolerance, withdrawal, cross-sensitization, cross-dependence, reward and opioid effects. Sugar addiction appears to develop as a result of natural endogenous opioids released upon sugar consumption. The opioid-like pain reducing properties of sugar are evident from birth. A sweet solution placed in a newborns mouth, elicits facial relaxation, often accompanied with a smile. Furthermore, something sweet placed on the tongue of a crying newborn produces an instantaneous calming effect. In another study, sucrose consumption delayed pain reporting in children aged 8 to 11 years old undergoing a cold-induced pain stimulus test, whilst having no effect in adult. Evolutionary driven taste preferences, coupled with heightened response to natural endogenous opioids produced upon sugar consumption make infants and children more vulnerable to sugar addiction than adults.
While it may not be reasonable to eliminate sweet foods entirely from a child’s diet, substitution of sugar with an all-natural sweetener such as vitaSWEETis a practical approach to abate the rising trends in childhood obesity and other detrimental health ailments associated with added sugar consumption. vitaSWEET is as sweet as sugar, zero calories, has no effect on blood glucose levels, and is safe for children.
References:
NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 175 to 2016: a pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet, 390 (2017), pp. 2627-2642
Herrick KA, Fryar CD, Hamner HC, et al. Added Sugars Intake among US Infants and Toddlers. Journal of the Academy of Nutrition and Dietetics. 2019.
Wang, Y., Guglielmo, D., and Welsh, J.A. Consumption of sugars, saturated fat, and sodium among US children from infancy through preschool age, NHANES 2009-2014. Am J Clin Nutr. 2018; 108: 868–877
US Departments of Health and Human Services and Agriculture. 2015-2020 Dietary Guidelines for Americans, 8th edition.
Nutrition and the Prevention of Chronic Diseases: Report of a Joint WHO/FAO Expert Consultation. World Health Organization, Geneva, Switzerland; 2004
Millen, B.E., Abrams, S., Adams-Campbell, L. et al. The 2015 Dietary Guidelines Advisory Committee scientific report: Development and major conclusions. Adv Nutr. 2016; 7: 438–444
Johnson, R.K., Appel, L.J., Brands, M. et al. Dietary sugars intake and cardiovascular health: A scientific statement from the American Heart Association. Circulation. 2009; 120: 1011–1020
Ventura, A.K., Mennella, J.A. Innate and learned preferences for sweet taste in childhood. Current Opinion in Clinical Nutrition and Metabolic Care. 2011. 14(4): 379-384.
DiNicolantonio, J.J., O’Keefe, J.H. Sugar addiction: is it real? A narrative review. British Journal of Sports Medicine. 2017. 52(14): 910-913
Mennella, J.A., Bobowski, N.K. & Reed, D.R. Rev Endocr Metab Disord. 2016. 17: 171.
“While it may not be reasonable to eliminate sweet foods entirely from a child’s diet, substitution of sugar with an all-natural sweetener such as vitaSWEET is a practical approach to abate the rising trends in childhood obesity and other detrimental health ailments associated with added sugar consumption.”
